Tonsils and Adenoids
Tonsils and Adenoids
Information about Tonsils and Adenoids

The tonsils form a ring of tissue around the throat known as Waldeyer’s ring. Tonsil tissue is found at the back of the nose and in the throat, which is known as the pharynx. This has 3 parts: the nasopharynx (back of the nose), the oropharynx (back of the mouth) and the hypopharynx (just above your voice box). There are 3 different areas of tonsillar tissue, known as lymphoid tissue, that make up your tonsils. Adenoids are found at the back of the nose; the palatine tonsils are the ones you see on either side at the back of the throat and the lingual tonsils are found on the back one third of the tongue, dropping down into the throat. Please see the photographs below identifying 3 areas of tonsil tissue.
Palatine tonsils
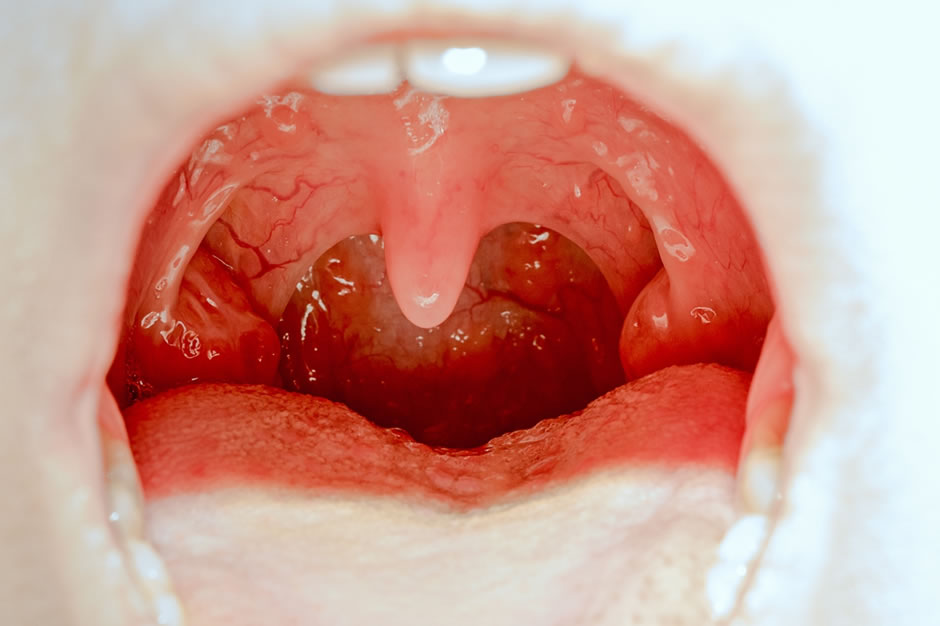
The palatine tonsils are the ones which are generally known as “your tonsils” – see below. They are easily visible by simply looking at the back of the throat where they sit on either side of the dangling bit in the centre of the throat – known as the uvula. They are usually pale pink and can be of varying sizes from very small and difficult to see to occupying nearly all the space in the back of the throat (see image below). There are a number of conditions that can affect the tonsils or be caused by the tonsils. Depending on the condition, they can either be managed conservatively with medication or by a surgical procedure.
Tonsil Pathology
Tonsillitis
Tonsillitis is an infection of the tonsils. Most tonsil infections are caused by viruses but they can also be caused by bacteria. There are lots of viruses and bacteria which cause tonsillitis. The tonsils will appear enlarged, red and inflamed and may have white pustules on them (see image below). They will be sore, you may have a temperature and swallowing can be difficult. Initial treatment for tonsillitis includes simple painkillers and mouthwashes. Antibiotics are usually only given if the tonsillitis is thought to be bacterial and this will be based on an examination by your doctor. If you suffer with recurrent tonsillitis, you may be offered surgery to remove the tonsils and prevent further infections. Within the NHS there are strict criteria as to who may have their tonsils removed for tonsillitis. Locally, we use the Scottish Intercollegiate Guideline Network recommendations and these can be accessed here. They recommend Tonsillectomy for recurrent tonsillitis if you have seven episodes in one year, four for two years in a row or three episodes three years in a row. This often leads to a lot of time off work or away from education and many people may want or choose to have their tonsils removed earlier.

Obstructive Sleep Apnoea
Enlarged tonsils can cause snoring or sleep apnoea – which is when the tonsils obstruct breathing during sleep. This can affect both adults and children.
Paediatric sleep disorders range from simple snoring to full-blown sleep apnoea, where breathing is restricted. Breathing may pause temporarily, and a child may wake gasping at night. Based on the history or if there is doubt about sleep apnoea, a Sleep Study may be required to show the presence of sleep apnoea in children. This usually only requires a monitoring of oxygen levels overnight. If a child has sleep apnoea with enlarged tonsils, we would recommend having them removed as sleep apnoea in children can cause a number of issues such as poor concentration, behavioural problems, reduced brain development – and in extreme cases – strain on the heart. If we were removing the tonsils for sleep apnoea, we would also inspect the adenoids to see if these are enlarged and potentially remove them as well. Sleep apnoea can occur with small tonsils as the adenoids alone maybe enlarged so if sleep apnoea is suspected it is always worth consulting a specialist.
Adults are managed slightly differently with regards to sleep apnoea. Having sleep apnoea as an adult can have a significant impact on quality of life. We can assess the impact this is having via various scoring mechanisms; and we would also want to see a patient in clinic to assess and offer treatment. Effects of adult sleep apnoea include an increased risk of cardiovascular problems such as high blood pressure and stroke, daytime sleepiness and feeling constantly tired. Removing the tonsils and adenoids may help with snoring in adults, but there is less evidence for sleep apnoea, unless they are very large when surgery would be combined with a Palatoplasty (removing the uvula at the back of your throat). Adults require a formal Sleep Study to assess whether they have sleep apnoea. My first line treatment for simple snoring would be with a mandibular positioning device rather than surgery and the best treatments for sleep apnoea are often conservative or medical with CPAP (high pressure air via a facemask when asleep). Very occasionally, straightening of the nasal septum (a Septoplasty) may be needed to help the high pressure air flow freely through the nose). There is also increasing evidence for tongue base surgery which can be discussed at your consultation.
Quinsy
A quinsy is also known as a peritonsillar abscess. It is when an abscess forms behind the tonsil and the wall of the throat. It is incredibly painful, which may affect the ear and often causes people to stop eating and drinking. Patients have an altered voice and a temperature. There would be swelling of that side of the throat and soft palate, often pushing the uvula off to the opposite side. This is treated with drainage of the pus and antibiotics. If a patient has episodes of quinsy, we would recommend that the tonsils are removed.
Asymmetrical Tonsils
Some tonsils are different in size, and these should be examined by a specialist. Most people with tonsils of different sizes have nothing to worry about. However, depending on what they look like as well as considering the individual case, we may recommend they are removed and examined to make sure there are no underlying problems. Asymmetrical tonsils may be a sign of a throat cancer and if you notice this you should be assessed by an ENT surgeon.
Tonsil Cancer
Cancer of the tonsils is on the increase due to human papilloma virus infection. It would usually present with a mass in the tonsil or at the back of the throat but could present with a lump in the neck, problems opening the mouth, a sore throat or earache. If patients have these symptoms, we would recommend an assessment by an ENT specialist. Patients with suspected tonsil cancer should be managed and treated within a Head and Neck Multidisciplinary Team (of which we are members).
The Procedure: Tonsillectomy
A Tonsillectomy is the procedure to remove the palatine tonsils. It is a very common procedure routinely performed within the ENT speciality. The procedure is done under a general anaesthetic and we always remove both tonsils. The procedure can be done in two ways; either an intracapsular tonsillectomy or extracapsular tonsillectomy. Depending on a number of factors, the patient may be offered one or the other or given the choice of which they receive.

Intracapsular Tonsillectomy
An Intracapsular Tonsillectomy is a newer technique which involves dissolving the tonsil using a technique called Coblation. This dissolves the tonsil tissue to make it disappear but leaves the capsule (a fibrous outer layer) within the throat. The benefits of this procedure are that it is less painful (and children are often back to school in less than a week) and has a lower risk of bleeding after the operation (less than 1%) with a very low chance of having to go back to theatre as an emergency over the first two weeks. The negative is that there is a small chance of tonsil regrowth which has been reported to be as high as 10% and can lead to a need for a second operation (in our practice this is very rare as we are incredibly careful to remove all the tonsil tissue). This procedure would be recommended for children with sleep apnoea and can be used for recurrent tonsillitis. In our experience, the Coblation technique is less effective in adults.
Extracapsular Tonsillectomy
An extracapsular tonsillectomy involves removing the tonsil and its capsule (the outer fibrous layer). It is more painful and needs two weeks off work/school. The risk of bleeding is increased and is quoted at around 5% over the two week post-operative period and admission to hospital for observation. Around 1% will need to have an emergency operation to stop the bleeding, however there is no risk of regrowth. This procedure will be performed for recurrent quinsy, asymmetrical tonsils, or suspicion of cancer (unless the cancer obvious and a biopsy would then be performed).
Tonsillectomy – risks of surgery
- Both procedures can cause pain (a Tonsillectomy is more painful the older you get)
- Post-operative bleeding which can occur up to 2 weeks later and if it occurs you should go straight to A&E
- An infection in the throat which may cause a foul smell or increasing pain and is managed with antibiotics.
- There is a small chance of damage to the teeth (usually already wobbly in children or diseased in adults)
- A stretched jaw which will settle over a few weeks or a small cut to the lip/gums which will heal very quickly without any intervention.
Post-operative information
Following the operation, you should rest at home (one week for intracapsular tonsillectomy, two weeks for extracapsular). You should take regular pain killers even if not in pain as it is harder to manage if the throat becomes painful. We advise you to eat and drink as normally as possible but avoid acidic or spicy foods as these will sting the throat. Eating and drinking reduces the chance of post-operative infection and bleeding. The back of your throat will go yellow/white – this is normal as it is a wet scab on the back of your throat. If the pain increases or you develop bad breath this may be a sign of infection for which you will need antibiotics. If you have any bleeding where you are spitting out blood beyond a little pink or blood-stained saliva, or spitting out a single clot, you should attend A&E immediately or call an ambulance. Children may swallow blood rather than spitting it out so if they seem off colour, are swallowing a lot or they complain of feeling sick/vomit blood please seek medical advice. If you have any questions following your surgery, please contact our Practice Manager and we will endeavour to help.
Adenoids

The adenoids are found at the back of the nose and can cause a number of conditions including snoring, sleep apnoea, nasal blockage, glue ear, ear infections, muffled hearing and eustachian tube dysfunction (pressure sensations in the ear). Depending on the cause, they can be removed which is done through the mouth so there are no scars.
See image below of the post nasal space after removal of adenoids.

Enlarged Adenoids
Enlarged adenoids can contribute to or cause sleep apnoea by blocking the nasal passageways when asleep, leading to difficulty in breathing or temporary pauses in breathing. Sleep apnoea in children can cause poor concentration, behavioural problems and reduced brain development. In extreme cases, sleep apnoea can cause a strain on the heart; and we would therefore recommend surgery with an Adenoidectomy (with or without Tonsillectomy) if there was a suspicion of enlarged adenoids causing sleep apnoea. Sleep apnoea in adults can cause cardiovascular problems such as high blood pressure and an increased risk of stroke, daytime sleepiness and feeling constantly tired. Enlarged adenoids in adults can easily be seen by passing a small camera to the back of the nose. But if there is doubt in children or it is unclear if the adenoids are enlarged, we can request a sleep study to look at a child’s overnight oxygen levels and breathing pattern; or have a look at the back of the nose – either under a general anaesthetic (and proceed to remove the adenoids); or if the child would tolerate it, we could pass a small camera through the nose to have a look at the back of the nose.
Adenoids, Adenoidectomy and ear related symptoms are discussed on the glue ear and ear infection pages of the website.
Adenoidectomy – risks of surgery
An Adenoidectomy is performed under a general anaesthetic and like any operation, the risks include:
- Pain (requiring simple pain killers)
- Bleeding – there is a very small risk that bleeding could start at any point for up to 2 weeks after the operation. If this is the case, we would recommend attending A&E immediately.
- Infection – identified by a bad smell or increasing pain and is managed with antibiotics.
- There is a very small chance of damage to the teeth (usually already wobbly in children or diseased in adults)
- A stretched jaw which will settle over a few weeks
- A small cut to the lip/gums which will heal very quickly without any intervention.
Post-operative information
Following the operation, you will need one to two weeks off (two weeks if combined with extracapsular Tonsillectomy). You should take regular pain killers and eat and drink normally. If your pain increases, or you notice a foul smell or you develop bad breath, this may be a sign of infection and you should be prescribed antibiotics. If you have any bleeding where you are spitting out blood you should attend A&E immediately or call an ambulance. Children may swallow blood rather than spitting it out so if they seem off colour, are swallowing a lot of complain of feeling sick/vomit blood, please seek medical advice. If you have any questions following your surgery, please contact our Practice Manager and we will endeavour to help.